Clinical Manifestation & Complications of loiasis
Loiasis has a variable clinical penetrance, ranging from asymptomatic over mild and unspecific to clinically distinct cardinal symptoms up to rare but potentially fatal organ impairments (2024).
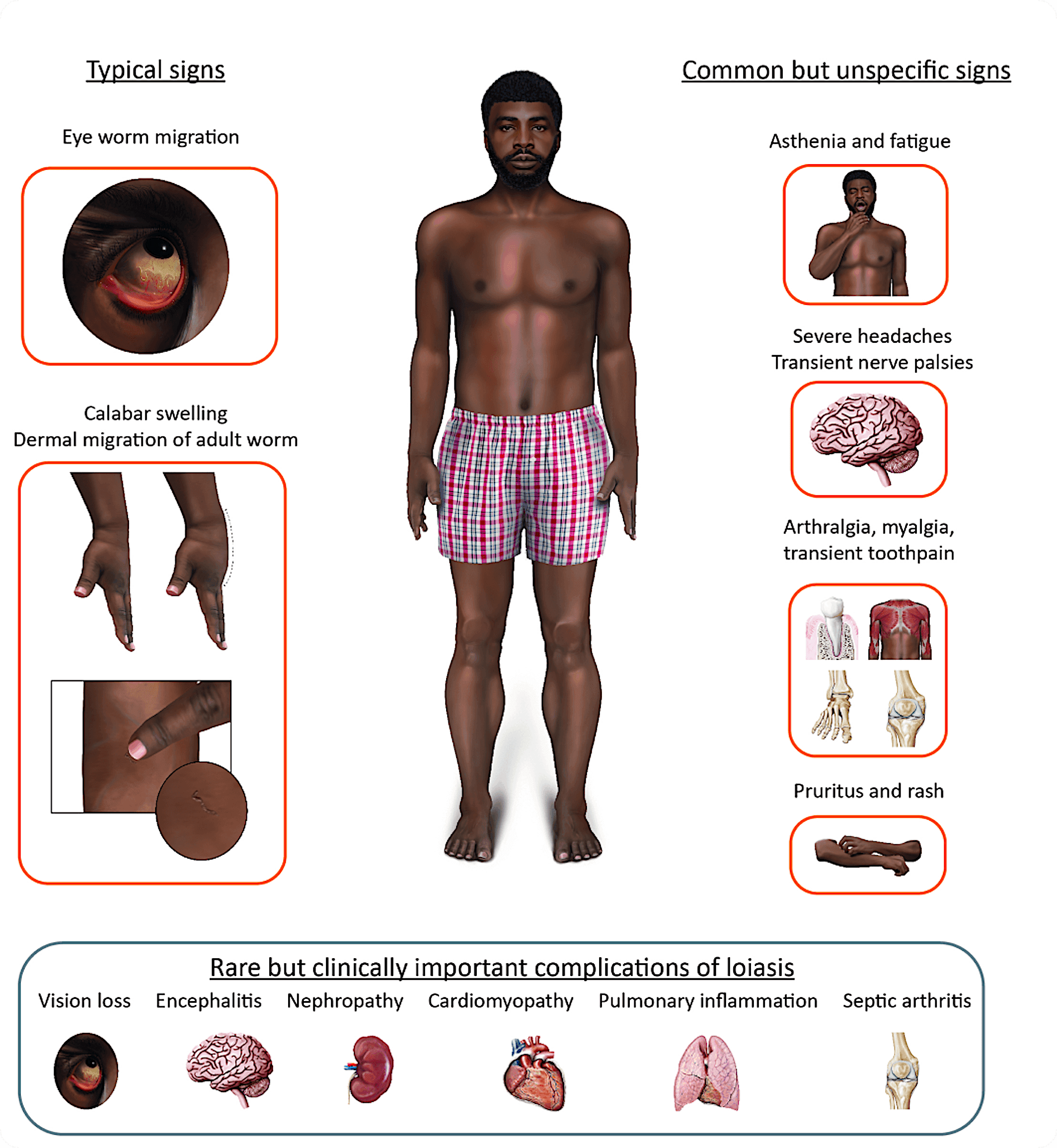
Pathognomonic signs and symptoms
Also being known as the African eye worm, the most frequent and distinct clinical sign of loiasis is the adult helminth’s migration through the eye’s subconjunctiva. Persisting over a time span of hours up to seven days, this can be accompanied by local itching, swelling, pain and increased sensitivity to light. The adult worm can be extracted comparatively easily during the migration through the conjunctiva.
The second cardinal symptom of loiasis is Calabar swelling. Due to an immunological reaction to the adult worm’s migration, a transient angioedema is formed. While mostly peripheral joints of the upper extremities are affected, Calabar swellings can occur in all parts of the body. As well as in the eye’s subconjunctival passage, Calabar swellings generally resolve without sequelae.
Common but unspecific symptoms
Even though fatigue, myalgia, arthralgia, cephalgia, temporary paralysis of peripheral nerves, paraesthesia, pruritus, rashes, urticaria and transient tooth aches are more unspecific, these mostly chronic symptoms represent the majority of the burden of disease. While many of these symptoms have been known for centuries, others have just recently been described scientifically (Paper toothache when published).
Clinical symptoms are rather associated with the migration of adult worms than the level of microfilaremia and was shown in endemic areas to correlate negatively with the level of microfilaremia.
Rare but potentially life-threatening complications
Encephalopathy and encephalitis are known complications following treatment regimens with DEC and ivermectin, even though cases without association to treatment have been described. Renal changes (hematuria and proteinuria) can be found, rarely leading to nephrotic syndrome and renal failure. High microfilariemia and hypereosinophilia can lead to endomyocardial fibrosis. Pleural effusions as well as ascites have been associated with loiasis.
References:
Ramharter M, Butler J, Mombo-Ngoma G, Nordmann T, Davi SD, Zoleko Manego R. Lancet Infect Dis. 2024 Mar;24(3):e165-e178. doi: 10.1016/S1473-3099(23)00438-3.
Veletzky L, Eberhardt KA, Hergeth J, Stelzl DR, Zoleko Manego R, Mombo-Ngoma G, Kreuzmair R, Burger G, Adegnika AA, Agnandji ST, Matsiegui PB, Boussinesq M, Mordmüller B, Ramharter M. PLoS Negl Trop Dis. 2022 Sep 19;16(9):e0010793. doi: 10.1371/journal.pntd.0010793.
Hildebrandt TR, Ramharter H, Lumeka Kabwende A, Endamne L, Davi SD, Adegnika AA, Mombo-Ngoma G, Agnandji ST, Mischlinger J, Manego Zoleko R, Ramharter M. Am J Trop Med Hyg. 2024 Jul 23:tpmd240059. doi: 10.4269/ajtmh.24-0059.